

Before services can be delivered, a client needs to access them. How does that happen? It seems straightforward enough: the Ministry of Health uses posters and perhaps radio spots to announce the service and where to get it. Then, clients who need the service will simply come. But it is rarely that easy. Just communicating information is often not enough to get clients to services.
Challenge
If people acted rationally based on what is proven to be best for them, everyone would avoid sugary snacks, immunize their children, get enough exercise and never start smoking. The truth is that people are not wholly rational actors; we make decisions based on our beliefs and emotions, even when those beliefs and emotions contradict overwhelming evidence. The challenge is to communicate effectively about a service in a way that motivates the desired behavior. People need not only to know about the service, but also to understand its value to them, feel like they can access it, know where to get it and feel able to navigate the barriers to access.
Barriers to access extend beyond individual knowledge, ability or attitudes. Relationships and communities can also influence individual willingness and capacity to go to health services. This could be through actively obstructing an individual or the general perception that the services are inappropriate or wrong. Lastly, external conditions such as physical or logistical barriers and gender and cultural norms can prevent service uptake.
Response
By using social and behavior change communication (SBCC) techniques rooted in behavioral science, service communication can inform and motivate individuals to access services and create an environment that promotes health-seeking behaviors.
Commercial marketing has long appreciated the power of emotion to sell products and services. SBCC has adapted commercial marketing techniques to go beyond demographics or behavioral data, seeking to understand why clients invest their time and money and associating services and health behaviors with client values and aspirations. Effective communication uses these insights in developing messages, selecting approaches and channels, and sequencing their delivery.
In using the socio-ecological model, SBCC recognizes the influence that a client’s environment has on decision-making. Family, friends and community all play a part in encouraging (or deterring) a client. At a higher level, policies can influence the availability of services, and advocacy – a component of SBCC – can be used to make services available.
The Demand Generation SBCC Implementation Kit provides a step-by-step process to build demand for key services and products.
Case Study: Audience Insight - VMMC in Zimbabwe
Challenge
Voluntary medical male circumcision (VMMC) is a priority for HIV prevention in Zimbabwe. The national policy aimed to reach 80 percent of 13- to 29-year-old Zimbabwean males (about 1.3 million young men) between 2011 and 2015. PSI provided technical and financial support to the Ministry of Health and Child Welfare to reach that goal. The program has 20 fixed sites, multiple outreach sites and mobile teams across all 10 provinces and offers VMMC through routine and campaign service delivery models. Launched in 2011, the Pinda muSmart (Get Smart) campaign positioned VMMC as a lifestyle choice of the smart, clean man. It used celebrity endorsements, appealing to trendsetters to be “ahead of the pack.” Despite this effort, results lagged. A World Health Organization progress brief calculated that by the end of 2014, Zimbabwe had circumcised more than 412,000—only 22 percent of the country’s target of 1.3 million men. This situation was not unique to Zimbabwe; many countries were falling short of their VMMC targets.
PSI has long used commercial marketing techniques – most of their products and services are branded for maximum appeal to the intended audience – and they conduct multi-level promotional campaigns using mass media and social mobilization to share their messages. But these techniques were proving inadequate.
Response
In a demand-creation meeting in 2013, the Gates Foundation engaged the market research firm Ipsos to work with the Ministries of Health in Zambia and Zimbabwe to gain insights as to why these well-executed campaigns were not achieving the expected results. The research sought to:
- Understand the decision-making process for men intending to undergo VMMC (including the impact of influencers)
- Identify physical and emotional drivers and barriers for VMMC uptake and the impact of the social environment
- Identify existing awareness, knowledge, perceptions and gaps related to VMMC
- Design a tailored communication and service approach for men seeking VMMC services
- Identify and map key stakeholders’ information gaps and use this research in the strategy
Barriers to Young People Accessing Sexual and Reproductive Health Services
Individual barriers – Lack of understanding of reproduction and sex. Desire to “become a woman or man” by having a child. Belief that healthcare is for women only. Poor experience/stigmatizing behavior by providers who believe young people should not access sexual and reproductive health services.
Community norms – Parents feel inhibited from talking about sexuality with their children. Belief among adults that talking about sex encourages promiscuity. Cultural norms that encourage early marriage for girls or cross-generational relationships.
Policy barriers – Condom distribution sales are restricted by age. National sexual and reproductive health curriculum is not comprehensive (abstinence based). Government does not prioritize youth as a key population for family planning. Policies require a woman to be married to access family planning.
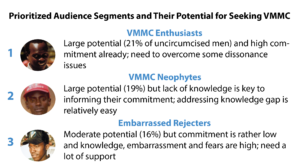
Qualitative country-level research enabled Ipsos to segment Zimbabwean men based on their level of awareness, belief and commitment to action. In particular, they identified cognitive dissonance in many men who understood the benefits of VMMC and health-seeking behavior, but had not been circumcised. The research identified key factors that influence real action and, based on these factors, Ipsos quantified the potential opportunity for each group based on current circumcision rates among:
- VMMC enthusiasts
- VMMC neophytes
- Scared rejecters
- Embarrassed rejecters
- Highly resistant
In 2015, PSI convened a workshop to review the research and map out how best to utilize it. Based on the potential opportunities presented by each segment, Zimbabwe decided to prioritize VMMC enthusiasts, VMMC neophytes and embarrassed rejecters.
The PSI team identified common motivators between neophytes and embarrassed rejecters, who were collectively estimated to represent 56 percent of uncircumcised men. Because the research went beyond gathering the typical demographic data (e.g., age, education, geographic location) and explored men’s unique values, motivations and feelings often not captured in formative research, the resulting messages for mass media, IPC and advocacy, were based on the functional and emotional benefits identified for each group.
In other words, the research asked potential clients what they believed the utility – functional benefits – of VMMC would be (e.g., reduced risk of HIV infection), as well as what positive feelings they associated with VMMC (e.g., feeling sexually attractive or feeling like a responsible sexual partner).
In the past, PSI used its highly trained researchers to collect additional information in the field and bring it back to the SBCC experts, who would design messages through a marketing strategy design workshop called “Delta.” The draft messages would then be pre-tested and rolled out at a national level. Using a new approach, PSI employed techniques adapted from human-centered design to develop strategies and messages. The PSI team shadowed their intended audiences, spending time with them to observe an average day’s routine.
Results
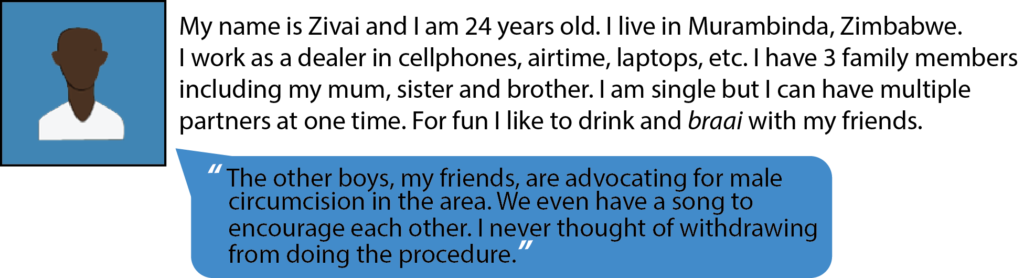
Zivai's values:
- He's strongly motivated by the "sex drive" benefits of getting circumcised
- He's very concerned about how his life will change after the procedure
- Sees himself as a "leader of the pack" and has strong social support behind him
Market research, combined with the human-centered design process, has enabled the PSI marketing and communication team to develop archetypes based on attitude and behavior toward VMMC. The image above offers an example of an “enthusiast” archetype.
Field staff are adapting a tool created during the research (a series of questions set up like a decision tree) to quickly segment clients into archetypes. This typing tool allows mobilizers to tailor their messages most persuasively. The tool, which is based on psychographics rather than typical demographic data, uses color-coded guidance to help mobilizers categorize each potential client into one of the key segments and then tailor messages that speak to the specific motivators and barriers of each segment. This helps ensure that one-on-one and small-group interactions are more efficient and effective in addressing the real needs of men.
The tool uses colors instead of segment labels (e.g., blue instead of “VMMC neophyte”) as an internal guide for mobilizers. This system has been piloted since February 2016 with plans for national rollout in July. Community mobilizers report that the approach has made their efforts more efficient. They no longer have to give a whole speech, but can confidently start with a few highly effective messages based on the potential client’s segment.
Ipsos’ research noted common themes among the determinants of VMMC-seeking behavior among men. One was the importance of former clients’ becoming VMMC champions and advocating for the service among their peers. Unfortunately, very few men were converting to VMMC champions after receiving the procedure. Another common barrier noted in the research was that messages minimized discussion of the pain men would experience, both during the procedure and throughout the healing process. Further probing found that some clients were surprised when they did feel pain and felt deceived. This left them less likely to advocate with their friends to go for circumcision. Because word of mouth was identified as a powerful way to get men into VMMC services, it was important to address the issue of pain directly. Using human-centered design approaches, the PSI team brainstormed around this challenge, creating prototypes and testing them with clients. Using feedback and input from real men, the Pain-o-Meter job aid was born. The Pain-o-Meter allows mobilizers to talk honestly about pain so potential clients have clearer expectations about pain during the procedure and in the healing period.
The Ipsos findings also indicated that if men became champions, they preferred to use their own words to describe their experiences. They asked the researchers to provide triggers rather than messages. Clients suggested that a mug or cap could be a conversation starter that allows the champion to tell his story, describe why circumcision was important to him, and talk about its benefits.
Engagement of field-level workers and the clients provided PSI with invaluable feedback to optimize the effectiveness of their tools and messages. PSI has begun to embrace the concept, popular in design work, of “failing fast,” which refers to using prototypes and iterative development to allow for rapid adaptation based on feedback and experience. Prototypes, which are simple, rough, facsimiles of the tools, materials or experiences, are taken out and used (rather than pre-tested with a focus group). Prototypes differ from a pre-tests in that the materials are far less fully formed and the ideas can go through major changes and transformations, even being thrown away entirely, without large sunk costs for design and human resources. The prototyping process also allows messages to go through constant adaptation as the experiences and needs of the mobilizers and clients are better understood.
Application
Understanding the intended audience is critical to effective communication, not just to understand their barriers and motivators, but also to empathize with their situations and engage them in finding solutions. Large-scale research can provide good documentation, and solid data can provide trends and rates, but careful observation, curiosity, and empathy can generate even deeper insights that allow for co-creation of effective messages and tools.
What is Human-Centered Design?
Human-centered design is a creative approach to problem-solving … that starts with the people you’re designing for and ends with new solutions that are tailor made to suit their needs. Human-centered design is all about building a deep empathy with the people you’re designing for, generating tons of ideas, building a bunch of prototypes, sharing what you’ve made with the people you’re designing for, getting their feedback and consistently refining and reiterating, and eventually putting your innovative new solution out in the world.
Human-centered design consists of three phases. In the Inspiration Phase you’ll learn directly from the people you’re designing for as you immerse yourself in their lives and come to deeply understand their needs. In the Ideation Phase you’ll make sense of what you learned, identify opportunities for design and prototype possible solutions. And in the Implementation Phase you’ll bring your solution to life, and eventually, to market. Throughout the work, you’ve kept the very people you’re looking to serve at the heart of the process. More
Additional Resources
Demand Generation I-Kit for Underutilized, Life Saving Commodities
Field Guide to Human-Centered Design
Male Circumcision Demand Generation Meeting Report. January 2015. Bill & Melinda Gates Foundation.
Bukuku, M. Presentation from SBCC Summit. February 2016. How to Link Demand Creation and Health Services: Experiences from Tanzania.
EngenderHealth and Promundo. 2008. Engaging Men in HIV and AIDS at the Service Delivery Level: A Manual for Service Providers. The ACQUIRE Project. Washington DC: USAID.
Research Triangle Institute and Population Services International. 2014. Voluntary Medical Male Circumcision (VMMC) Demand Creation Toolkit. Washington DC: US Centers for Disease Control and Prevention.
Sutton, SM, Baich GI, and Lefebvre RC. nd. Strategic Questions for Consumer-Based Health Communications.