

 SBCC and service delivery partners collect routine program data. This information is most useful to service delivery if it is collected in a timely fashion to allow for rapid changes that can improve the program’s effectiveness. The information gathered through routine monitoring may include client feedback on providers and services, insights on perceptions of service quality, levels of provider stigma, gaps in linkages and referral systems, changes in beliefs and attitudes among providers or clients, and effective demand-creation channels and techniques.
SBCC and service delivery partners collect routine program data. This information is most useful to service delivery if it is collected in a timely fashion to allow for rapid changes that can improve the program’s effectiveness. The information gathered through routine monitoring may include client feedback on providers and services, insights on perceptions of service quality, levels of provider stigma, gaps in linkages and referral systems, changes in beliefs and attitudes among providers or clients, and effective demand-creation channels and techniques.
Collecting this information is important for service communication because it can be used to make the following types of program changes:
- Determining whether effective referrals are being made and, if not, how messaging can address gaps – For example, do referred clients represent the intended audience? Are they adequately informed about key information about the service once they arrive?
- Modifying the content of counseling sessions/job aids to address clients’ questions or concerns about the service or health area – In Zimbabwe, for example, routine client satisfaction surveys revealed dissatisfaction in how VMMC providers talked about pain during the clinical encounter. This decreased the likelihood that men who received the service would recommend it to others. A new job aid, the “Pain-o-Meter,” was prototyped to help providers communicate pain expectations more accurately.
- Modifying or changing channel selection, intensity or frequency – Routine monitoring data including clinic records and counseling feedback can provide information about which communication channels are driving service uptake the most. For example, do clients come because of a radio spot, community-based activities, peer agents? This information can help programs to realign resources to change the intensity or frequency of various channels or discontinue those that don’t result in any clinic visit.
- Improving personnel decisions, provider support supervision and coaching strategies – Routine client feedback and observation can indicate any concerns clients may have with providers. These concerns could include discomfort with the types of personnel providing service (for example, male VMMC clients are uncomfortable with female providers, youth prefer younger providers) or the ways in which providers engage with the client. While personnel changes may not be possible, feedback can be used to develop routine support supervision and coaching systems to improve provider behavior.
In order to act on this information, SBCC and service partners should regularly review service statistics and client feedback to identify performance gaps and opportunities for improvement. This can be done through regular meetings to review monthly or quarterly reports on community activities and service statistics.
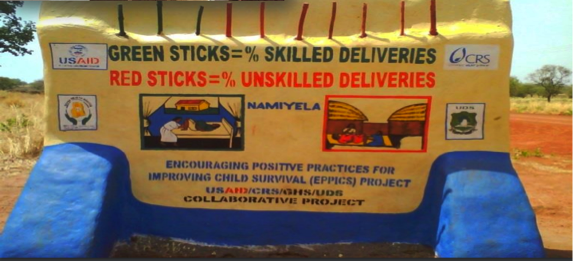
In Ghana, the EPPICS project created giant community scoreboards to track performance against maternal and child health indicators. Each month, they update the scoreboards with green (positive outcome) or red (negative outcome) sticks to show how the community is doing. In addition to monitoring progress, the scoreboards also help educate community members about healthy practices and motivate community members to adopt healthy behaviors.
In its VMMC demand-creation program in Tanzania, Jhpiego learned from routine monitoring data that if providers talked about the importance of follow-up after the procedure, they experienced a considerable spike in clients’ attending follow-up visits (the wanted at least 80% of all VMMC clients to return for follow up care). Jhpiego used real-time data gathered from clinic records and observing counseling sessions to conduct supportive supervision visits that focused on improving that one behavior – getting providers to discuss the importance of follow-up with every client.
The project also used routine clinic data summarized in a data dashboard to communicate to peer mobilizers how they were performing against monthly demand-creation targets. The dashboards were displayed in the health facility and reviewed by each facility team on a weekly basis and at annual regional data summits. This data also guided quarterly support supervision visits with regional and national representatives from the Ministry of Health. During these meetings, the project team regularly reviewed the dashboards for the number of monthly VMMC services provided, the number of adverse events and the number of follow-up visits. Collectively, they then identified opportunities for improvement and celebrated successes.